A 65-year-old woman with a history of rheumatoid arthritis presented with neck pain, frequent falls, and difficulty with fine motor movements of the hands. On neurological exam, she had full strength but had 3+ reflexes in the upper and lower extremities and positive Babinski and Hoffman signs.
A magnetic resonance image (MRI) of the cervical spine demonstrated a pannus formation at C1–C2 with mild ventral cord compression and T2 signal change. Additionally, lateral flexion-extension radiographs demonstrated 8 mm of translation of C1 with respect to C2. She was recommended to undergo a C1–C2 decompression and C1–C2 arthrodesis, but declined the operation.
She neglected to follow-up but presented 2 years later with increased weakness, particularly in her upper extremities. Additionally, she had been treated for multiple episodes of aspiration pneumonia. On neurological exam, she had 3/5 strength in her bilateral upper extremities, and 4–/5 strength in the bilateral lower extremities. She had 3+ reflexes in the bilateral upper extremities, and 4+ reflexes with clonus in the Achilles reflex bilaterally
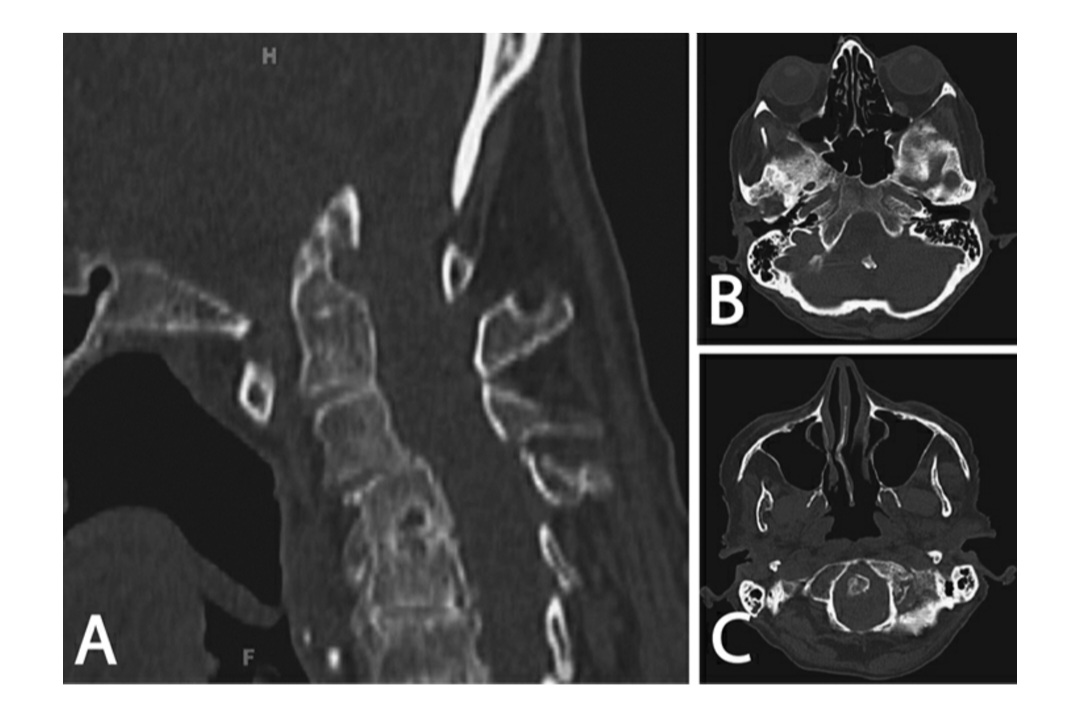
A computed tomography (CT) image demonstrated new upward translation of the odontoid with extension of the tip of the odontoid 14 mm above the McGregor line (A) . (A) Sagittal computed tomography (CT), (B) axial CT of the posterior fossa, and (C) axial CT at the level of the foramen magnum demonstrating basilar invagination with significant upward translation of the odontoid into the posterior fossa.
Questions:
1.What is the likely diagnosis?
2.How are basilar impression, basilar invagination, cranial settling, and platybasia defined and distinguished?
3.What imaging modalities should be utilized to assess these patients?
4.The presence of what other occipitocervical (OC) pathologies should be assessed?
5.What other disorders are frequently associated with OC pathologies?
Case Discussion
Assessment and Planning
The neurosurgeon suspects a diagnosis of basilar impression with cranial settling due to progression of the patient’s C1–C2 instability from rheumatoid arthritis. Basilar impression, basilar invagination, cranial settling, and platybasia are often used synonymously, but they represent discreet terminology.
(Reference Smith et al, 2010). 1 Basilar impression represents the broader category of OC junction pathologies. Basilar invagination results from migration of the entire spine into the skull base as the skull base remodels or invaginates (Figure), usually from congenital hypoplasia or dysplasia of various osseous structures at the OC junction or achondroplasia. Common pathologies leading to basilar invagination include osteogenesis imperfecta (most commonly type III), disorders of bone metabolism such as Paget disease, rickets, and hyperparathyroidism. In osteogenesis imperfecta, the load-bearing capacity of the skull base is exceeded with microfractures in the region of the foramen magnum, leading to gradual deformity and softening of the skull base. OC junction tumors, trauma, and infection can lead to basilar invagination, but usually result in cranial settling. Cranial settling is a form of basilar impression due to C1–C2 instability (commonly in the setting of rheumatoid arthritis), defined as upward migration (or rotation) of the C2 complex into the cranial vault. Atlanto-occipital assimilation can develop into cranial settling, with ligamentous laxity at the C1–C2 level that develops over time. This laxity may result from stress on the C1–C2 complex from assimilation of the condyles and C1. The lack of flexion-extension at the craniocervical junction leads to stress at C1–C2 that ultimately results in the cranial settling. Platybasia is simply deformation and flattening of the skullbase that can be found alone or in combination with other OC pathology.
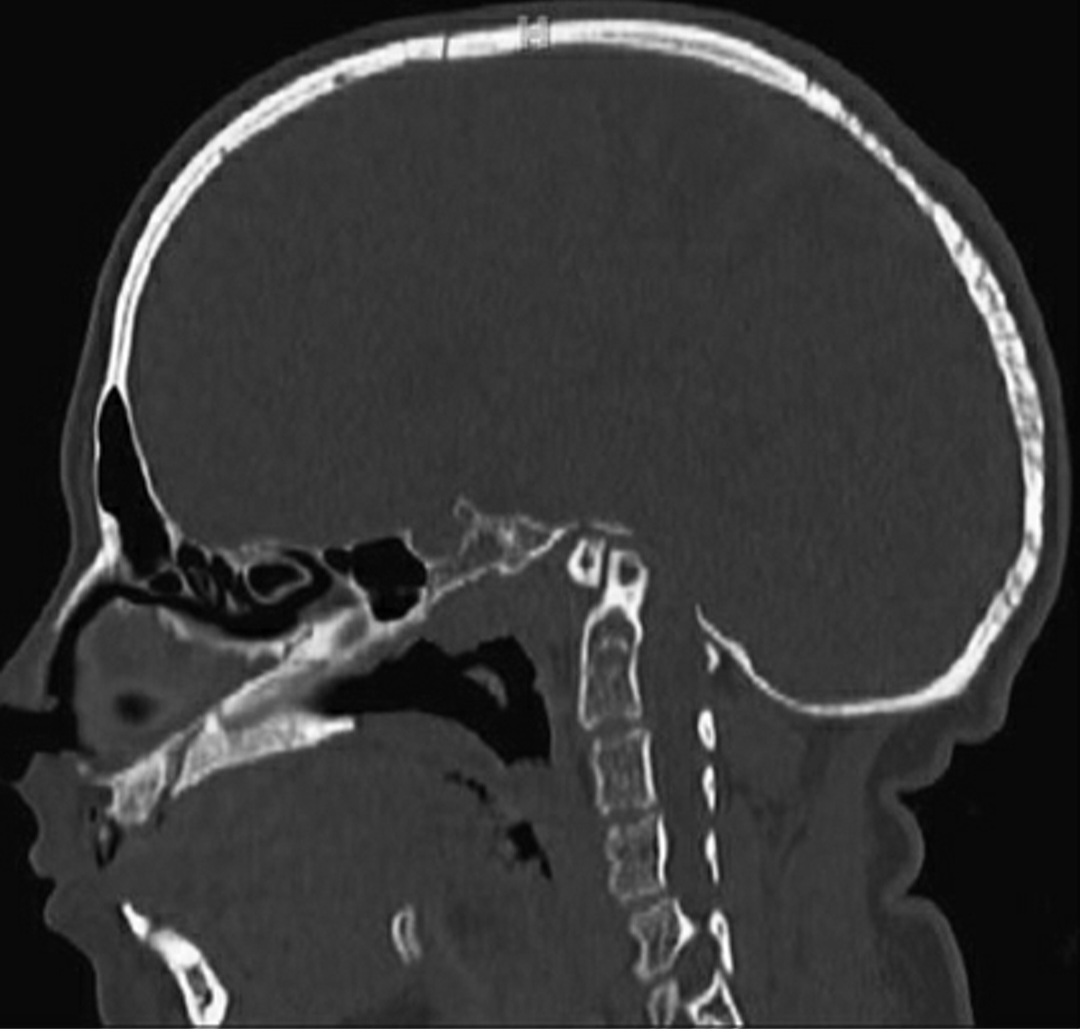
Sagittal computed tomography (CT) scan of a patient with osteogenesis imperfecta demonstrating basilar invagination with upward migration of the C1–C2 complex into the cranial vault
Patients with basilar invagination frequently have concurrent Chiari type I malformations, with rates of 54% reported in a series of 190 patients.2 In this series, most patients presented between the second and fourth decades of life, with earlier and more acute presentation in patients without a concurrent Chiari type I malformation. Many patients reported neck pain, and common physical exam findings in both groups included myelopathy with weakness and paresthesias, gait abnormalities, bowel and/or bladder dysfunction, short necks, webbed necks, and lower hairlines. Additionally, patients may present with lower cranial nerve dysfunction depending on the extent of brainstem compression.Basilar invagination was historically identified on open-mouth anteroposterior (AP) plain film radiographs in which the C1–C2 facet complex was incompletely visualized. More detailed assessment can be made by determining the relationship of the odontoid tip with the Chamberlain line and McGregor line. Basilar invagination is typically diagnosed with extension of the tip of the odontoid at least 5 mm above the Chamberlain line or more than 7 mm above the McGregor line. Cranial settling is identified with protrusion of the tip of the odontoid more than 4.5 mm above the McGregor line in the setting of rheumatoid arthritis. Currently, CT images with sagittal, coronal, and three-dimensional reconstructions are ideal for characterizing and defining OC junction abnormalities, particularly as these patients often have complex osseous anatomy with potentially Klippel-Feil and/or cranial assimilation of C1. Additionally, MRI is critical for assessment of neurologic structures and spinal cord and/or brainstem compression, as well as soft tissue and ligamentous structures. Flexion-extension radiographs can be used to assess for instability, though caution should be exercised in the setting of often severe spinal cord and brainstem compression. Finally, vascular imaging such as CT angiography or even four-vessel cerebral angiography is useful to define the vertebral artery anatomy, which may have an aberrant course in the setting of craniocervical pathology.
Board Exam Pearls
Diagnostic Pearls
1.Radiographic imaging with CT scans or lateral radiographs is used to differentiate basilar invagination and cranial settling.
a.Basilar invagination: Upward migration of the entire spine into the skull base as the skull base remodels or invaginates.
b.Cranial settling: Upward migration (or rotation) of the C2 complex into the cranial vault in the setting of C1–C2 instability.
2.Each patient should undergo a detailed history and physical exam. Important historical information includes the length of the symptoms, progression of symptoms, and acuity of any changes change in neurological status, as well as presence of any medical comorbidities that may be associated. Important physical exam assessments include visual inspection, assessment of cervical range of motion, and performance of a detailed neurological exam including cranial nerve assessment.
3.Performance of CT imaging of the craniocervical junction is imperative for adequately assessing the potentially complex osseous anatomy.
4.Performance of MRI of the craniocervical junction is required to adequately determine the extent of compression of neurological structures, as well as assess the soft tissue and ligamentous structures.
5.Vascular imaging, typically with CT angiography, is important to adequately identify the vertebral artery anatomy, which may often have an aberrant course in these patient.
Questions:
1.What is the most appropriate timing for operative intervention?
2.How do the clinical and radiographic findings influence surgical options?
3.How should cervical traction be used to determine the optimal surgical strategy?
4.What is the importance of oral hygiene prior to surgical intervention?
5.What is the significance of preoperative nutritional status and pulmonary function?
Decision Making
If untreated, basilar invagination and cranial settling may lead to significant neurological deterioration and even death. Although no specific criteria for surgical intervention exist, most patients present with some degree of neurological compromise and will require surgical intervention with decompression and stabilization in order to prevent further neurological decline. However, a small subset of patients who present without neurological deficits and with minimal extension of the odontoid into the foramen magnum and no spinal cord or brainstem compression could be followed closely clinically. Before surgical intervention, many patients with basilar impression undergo a trial of cervical traction to determine the amount of reduction of the odontoid that may be achieved. However, significant caution should be exercised in patients with significant compression to prevent further neurological injury. In general, low weights (5–10 pounds) should be used with close neurological monitoring and the angulation of the traction modified to reduce neurological compression, often with the head elevated approximate 15 degrees above the horizontal plane. If the odontoid is completely reducible, the patient may be a candidate for posterior decompression and fusion alone.3 However, if the odontoid cannot be reduced, the patient often requires anterior decompression in conjunction with posterior stabilization (and often posterior decompression as well). There is a spectrum of severity of patients with cranial settling. Initially, there is C1–C2 instability, followed by C1–C2 instability with pannus formation. If left untreated, C2 starts to migrate upwardand pseudostabilization occurs, with regression of the pannus. This is followed by complete cranial settling. All of these patients require posterior stabilization, but the degree of stabilization is determined by where the patient lies in the spectrum of severity. For C1–C2 instability with or without a pannus, the patient can be treated with only C1–C2 instrumented fusion. For early migration of C2 with pseudostabilization, the patient can be treated with reduction and C1–C2 fusion, or OC fusion if the C1 lateral masses are destroyed. Finally, full cranial settling, if irreducible, requires ventral decompression and OC fusion. As anterior surgical approaches often involve a transoral approach, preoperative assessment of dental hygiene is critical to minimize bacterial contamination of the surgical field. Dental caries and gingivitis require treatment prior to surgery as these may result in hematogenous spread or surgical site infection with a risk of meningitis if a durotomy is encountered. Furthermore, loose dentition should be guarded or prophylactically extracted preoperatively. Also, patients often have lower cranial nerve dysfunction, particularly of the glossopharyngeal, vagus, and hypoglossal nerves. If there is significant dysfunction of these cranial nerves, preoperative tracheostomy placement should be considered. Additionally, patients may have concurrent swallowing dysfunction with resultant poor nutritional status. In these patients, preoperative placement of a percutaneous gastrostomy should be considered to optimize nutritional status preoperatively for improved wound healing. Finally, some patients, both children and adults, may have inadequate mouth opening to establish a sufficient surgical corridor, necessitating use of alternative approaches
Surgical Procedure with Video
Questions
1.What regions of the craniocervical junction can be approached with the different ventral approaches? 2.What is the significance of the presence of a pannus in terms of the surgical procedure?
3 Comments
Here is an example of a comment left.
Here is a second comment on this case. I have many comments to add here.
Phasellus porta dui commodo, accumsan nisl id, convallis nibh. Phasellus posuere lacus eget efficitur maximus. Phasellus eu porttitor risus. Cras et hendrerit metus, sit amet blandit tortor. Proin in risus purus. Cras tortor enim, volutpat eu dignissim quis, vulputate scelerisque mi. Donec iaculis, mauris nec sollicitudin vulputate, enim augue feugiat justo, ut pulvinar tortor sem a ipsum. Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Here is a comment with some rich text in it.
Lets link to alexleuschner.com
Title
Some text written in italics..